Mon - Thursday: 9.30am - 5.30pm - Most Saturdays - 9am - 1pm
Top 8 Uses of Low Dose Naltrexone (LDN) + Side Effects
A revolution in the background of medicine. Studies reveal it may help people with complex autoimmune diseases, chronic pain, inflammation, cancer, infections, and autism. Read on to understand its unique mechanism, potential uses, side effects, efficacy, and natural synergies.
WELL-BEINGNUTRITION SCIENCECANCER
Benjamin McAvoy
12/18/202422 min read
Top 8 Uses of Low Dose Naltrexone (LDN) + Side Effects
Low Dose Naltrexone causes various effects in human being. The serendipitous discovery of low-dose naltrexone (LDN) spurred a revolution in the background of medicine. Studies reveal it may help people with complex autoimmune diseases, chronic pain, inflammation, cancer, infections, and autism. Read on to understand its unique mechanism, potential uses, side effects, efficacy, and natural synergies.
Here is a link if you can not see the Video
What is Naltrexone?
Before the concept of low-dose naltrexone was born, high doses of this drug were used in conventional medicine for completely different purposes.
Naltrexone is a drug that blocks the activity of opioids in the brain – an opioid receptor antagonist. Your body normally produces endorphins and enkephalins, natural opioids that activate these receptors and contribute to feel-good sensations. They allow for a fear- and pain-free daily existence. In fact, these chemicals are the body’s most powerful reward and pleasure system [1, 2].
Opioid drugs can provide relief from chronic, intense pain. But they don’t come without risks: high doses can slow or even stop breathing and exaggerate feelings of calm, euphoria, and pleasure when abused. Opioid drugs include both prescription painkillers like Vicodin and Percocet, as well as drugs of abuse like fentanyl.
Although we are currently seeing the disastrous effects of the opioid epidemic – from doctors over-prescribing opioid painkillers to extremely potent opioids like fentanyl reaching the streets – the concept of reversing opioid activity dates back to a time before the present-day crisis began.
The opioid blocker naltrexone was synthesized in the 60s and approved in the 80s for treating opioid addiction [1].
Doctors gave naltrexone to opioid addicts in recovery in the hopes of preventing relapse. The rationale was to completely shut off the ‘high’ of abused narcotics. By blocking all receptors in advance, naltrexone renders narcotics powerless. The dosage needed to achieve opioid blockage is high, ranging from 50 – 100 mg/day [1, 3].
Disclaimer: Low Dose Naltrexone shouldn’t be confused with naloxone (Narcan), although both drugs are opioid blockers. You may have heard about naloxone kits (spray or injection) that can save lives in opioid overdose. Naloxone is a better choice for reversing overdose because it starts to act faster and lasts for a shorter time, as is desirable in emergency situations. Naltrexone, on the other hand, takes a couple of hours just to kick in [4, 5].
Snapshot
PROs
A promising alternative for autoimmune diseases, chronic pain, and inflammation
Low Dose Naltrexone Increases natural opioids
Balances the immune system
May help people with cancer (preliminary research)
Side effects are rare and mild
Very few known drug interactions
CONs
Off-label use
Dosing usually must be adjusted to each individual
Use largely relies on clinical expertise, not on large-scale studies
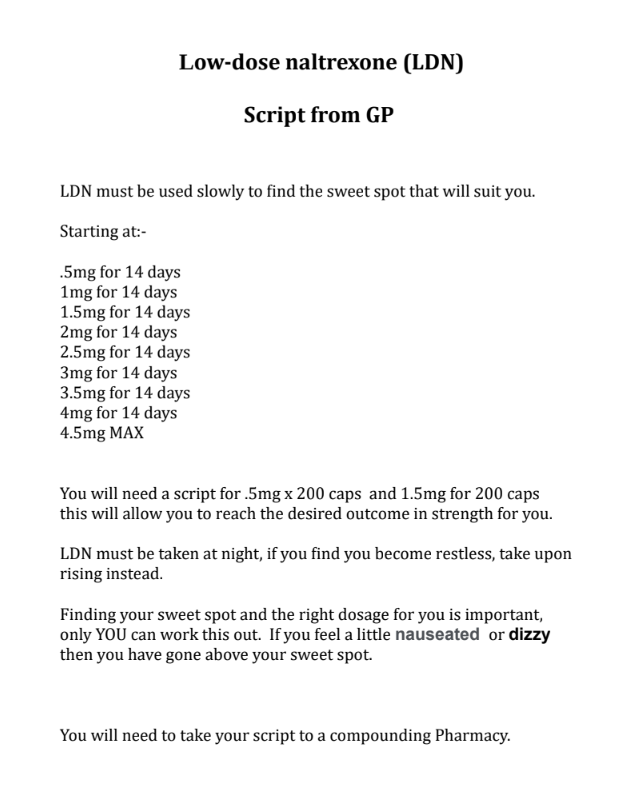
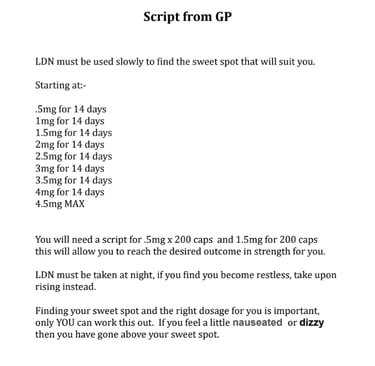
How to take LDN - ( See your GP or doctor for a script or more information.
The Discovery
Around the same time when naloxone was being used for opioid addiction in mainstream clinics, New York-based physician Dr. Bernard Bihari started using the drug in very Low Dose Naltrexone in the midst of the first AIDS epidemic. By attempting the impossible – using an opioid blocker to enhance the immune response in people with an ‘untreatable’ disease – Dr. Bihari spurred a lot of attention.
Knowledge about the effects of endorphins was just in the early stages when Dr. Bihari started experimenting with LDN. He was initially working with opiate addicts when he observed that high dose naltrexone makes the body triple endorphin production. However, it caused too many side effects, such as insomnia and the inability to handle stress. Few would stay on it.
To re-wind: your opioid-like endorphins are not only released to help you cope with everyday social situations free of fear, pain, and anxiety. They also play an important role in acute stress and the fight-or-flight response [6].
Imagine you are faced with a dangerous situation, as our ancestors were in front of a predator in the wild. Your body pours out endorphins along with cortisol and epinephrine. The endorphins will make you fearless if you need to fight, relieve pain during the fight, and boost your immune system to reduce the risk of infection and enhance wound healing if you get injured [6].
Interested in the drug’s immune effects, Dr. Bihari started prescribing a range of naltrexone doses to HIV patients. The goal was to find the best dose that would boost endorphins without causing negative effects. Surprisingly, it turned out that a small naltrexone dose (3 – 5 mg) increased endorphins to the same extent as a high dose [6].
Next, he ran a 9-month LDN trial in people with AIDS with promising results. After realizing the immune-normalizing benefits of LDN for AIDS, Dr. Bihari uncovered its application for a wide range of autoimmune diseases [6].
However, it wasn’t until 2007 that the first low-dose naltrexone (LDN) clinical trial was published. All the while, science has been gaining a lot of insight into the intricate workings of endorphins and opioids in the body. Other LDN studies have been published and the knowledge about its clinical use has grown, gaining attention as a potential treatment for many chronic diseases [1].
How Low Dose Naltrexone (LDN) Works
Low naltrexone doses block opioid receptors for a short time – about 3 hours. In response, your body increases the production of endorphins. LDN should be taken before sleep, as 90% of the endorphins are made in the middle of the night, between 2 and 4 AM. According to Dr. Bihari, a small late-evening dose of naltrexone will boost endorphin production by 300% [6, 1].
Although naltrexone is cleared away by the morning, endorphins stay high all the next day. The endorphin blockage from low dose naltrexone is mild, short, and essentially increases their activity. In comparison, high dose naltrexone does raise endorphins but keeps the receptors constantly blocked, reducing their activity as the end result [6, 1].
The rise in endorphin levels remains for as long as you’re taking the low dose every night.
Beta-endorphin, one of our main natural opioids, has a long half-life of about 20 hours in the body (half-life refers to how long it takes the body to clear half of it). It’s unknown for how long other endorphins that are harder to measure stay high in the blood.
This is important because the endorphins your body makes act on different opioid receptors. For example [6, 7, 8]:
Mu receptors are in the brain and help with pain relief.
Delta receptors are found in many tissues in the body and may play a role in controlling cancer and the immune system.
There are several other receptor types that may be important for the action of LDN, but these two play the largest role [1].
The Missing Link Between Cancer, Autoimmunity, and Depression
Taken from: Aristo Vojdani, Ph.D.: Mechanisms Associated with LDN Therapy in Autism and HIV
To understand why LDN may have such profound effects, we need to get to the bottom of how complex disease like cancer, autoimmunity, and mood imbalances are connected to endorphins.
Cancer and autoimmune diseases may be triggered by low blood levels of endorphins, which contributes to immune deficiencies. Similarly, HIV/AIDS is accelerated by a deficiency of endorphins. Of course, they are not the only cause, but they are a piece of the puzzle [7].
Another interesting concept that explains the brain-immune connection is the so-called “sickness response” or “sickness behavior”. When people are faced with a disease – be it cancer or depression – they will tend to isolate themselves, while the body will increase inflammation and alter the immune response [9].
To draw a parallel, sickness behavior is well-known to scientists in the animal world: animals will isolate themselves for a short period of time when faced with an infection or disease to avoid contaminating others.
It turns out that low endorphins may be the culprit of this complex psychological and emotional response in humans. Sickness behavior can become devastating if it stops to serve a purpose and turns into chronic low mood and energy. By boosting endorphins, LDN may help steer behavior away this type of response, while also balancing the immune system [9, 10].
To sum it up, LDN has the capacity to correct endorphin and enkephalin deficiencies. As a result, it boosts the immune system, fights inflammation, and reverses sickness behavior in disease.
Does It Block or Stimulate Endorphins?
The concept of “stimulating by blocking” is not an easy one. Let’s dive a bit deeper.
The hypothalamus is a structure in the base of the brain and part of the limbic system, which orchestrates emotions, motivation, and learning. Low-dose naltrexone blocks opioid receptors in the hypothalamus [6].
In response to the short-term blockage, the brain begins producing more of a prohormone called proopiomelanocortin during the night. Next, this hormone is broken up into 3 others in the pea-sized “master gland” called the pituitary:
Beta-endorphin
Melanin-stimulating hormone
Aside from these direct effects on the brain, LDN may also signal the adrenals to make more enkephalin via another prohormone called proenkephalin.
This is a normal response, as the body interprets blocked receptors as a signal that our endorphins are low. To compensate, it increases their production. For this reason, we can say that LDN increases our natural opioids – endorphins and enkephalins – by blocking.
Here we can again see how important the low dose concept is. If the receptors are blocked by a high dose, they don’t get to recover and stay shut off. According to Dr. Bihari, the ideal dose should maximally increase endorphins while minimally blocking them [6].
Is It Legal?
Despite the persisting scientific efforts, LDN is still thrown into the “alternative treatments” bucket. But that doesn’t make it illegal.
Naltrexone is a drug licensed and approved by the FDA, meaning that doctors can prescribe it. However, naltrexone is not approved in low doses or for the indications we focus on in this article. That makes the use of LDN “off-label”.
Off-label use is nothing unusual, though. Doctors sometimes prescribe drugs this way if they consider they can have benefits for patients outside the established indications – as is the case with LDN. Such use is completely legal and medically acceptable.
Uses of Low Dose Naltrexone
1) Autoimmune Conditions
Dr. Bihari first realized that LDN may help people with autoimmune diseases. According to him, LDN has the power to restore immune harmony by rebalancing T-helper cells, the so-called master cells of the immune system. People with autoimmune issues tend to have impaired T-helper cell function [6].
A specific subtype of these T-helper cells are Tregs (5% – 10%), which are responsible for suppressing harmful Th1, Th2, Th17 overactivation. Tregs are powerful cells that prevent the immune system from going into an autoimmune overdrive, or simply said, from attacking itself. Tregs can also reverse food intolerances and allergies [11, 12].
Two other important immune cells that come out of balance in people with autoimmune diseases are macrophages and killer cells. They stop being able to discriminate between the body’s own tissues and foreign invaders, which launches an autoimmune attack and raises inflammation. In multiple sclerosis, these start attacking the nerve-protective myelin sheath. As the attacks progress, so does brain damage and the accompanying symptoms.
Based on these findings, Dr. Bihari assumes that LDN works by enhancing the functioning of the T cells, which rebalances immune function and brings an end to the self-attack. Although clinical studies have yet to confirm his clinical findings, Dr. Bihari claims that LDN can help people with a range of autoimmune diseases including lupus, rheumatoid arthritis, eczema, and psoriasis.
The whole basis for these potential benefits stem from boosting endorphins, and their subsequent rearranging of cells in the immune system [6].
Research revealed that LDN also blocks the activation of microglia, a type of immune cell in the brain and nervous system. Microglia normally stay in a resting state and are woken up only by brain damage or infection. Their activation underlies common symptoms in autoimmune and other diseases (see “sickness behavior”): fatigue, fever, inflammation, and pain. Once blocked, their inflammatory products and toxic substances go down (possibly via blocking TLR4) [7].
The researched conditions are listed below. Beyond them, it’s possible that LDN may also help with other diseases with an autoimmune component such as Hashimoto’s. LDN is reported to work in people with Hashimoto’s. Anecdotally, it improves thyroid health, lowers antibodies and the need for additional drugs.
Multiple Sclerosis (MS)
At first, the evidence to support LDN use in MS seems conflicting. In one study of 96 people with MS, 8 weeks of LDN (4.5 mg/day) did not provide more relief than placebo. In contrast, LDN improved mental health and quality of life in another study of 60 people with MS, using a similar protocol. It is possible that 8 weeks is too short a time and that the doses need to be adapted to each person individually to see results [13, 14].
One study tracking back 4 women with MS suggested that LDN is safe and may help slow the disease. Women who took LDN didn’t report any side effects, while their symptoms stabilized or improved, as did their quality of life and fatigue [15].
Overall, clinical evidence suggests that LDN helps MS patients, while the scientific studies are less clear on its effects. Larger studies are needed to fully assess the benefits of LDN for MS.
Rheumatoid Arthritis
In 10 people with rheumatoid arthritis, LDN cleared joint pain and swelling. A few weeks after they stopped taking LDN, most experienced periods of severe stress and disease worsening [7+].
Fibromyalgia
Fibromyalgia is not technically classified as an autoimmune disease, although it triggers many of the same symptoms. Some scientists are fighting to show that fibromyalgia is autoimmune, while others think its a state of chronically heightened pain sensitivity. Either way, LDN seems to offer some hope for people suffering from this otherwise hard-to-treat disease [16, 17].
A group at Stanford University found that LDN (4.5 mg/day) significantly reduces pain, fatigue, inflammation, and stress levels in people with fibromyalgia, while boosting mood and happiness. In this clinical trial, LDN was extremely safe and well-tolerated. Participants rated the side effects similar to placebo [18].
Another small clinical trial uncovered that people with fibromyalgia have lower endorphins (or a “low opioid tone”). LDN reversed their low levels, thereby improving pain tolerance. Interestingly, it also enhanced the patients’ ability to relate interpersonally and engage in relationships. This goes a long way to show how profound of a physical and emotional effect endorphins can have [19].
Itchiness (and Possibly Histamine Intolerance)
In one interesting study, people underwent brain imaging (fMRI) to track how the brain responds to an itch caused by histamine and capsaicin – both trigger burning, stinging, or prickling feelings. However, when the participants were given LDN, the itching sensation went away, which was confirmed by lower activity in itchiness-linked brain regions [20].
Itchiness is also a common symptom in people with an autoimmune condition called scleroderma (systemic sclerosis) as well as in eczema and psoriasis, which explains why LDN may help [21, 22].
In another study of 3 women with scleroderma, LDN significantly reduced severe itching of the skin and gut symptoms. Skin itching and gut problems in scleroderma are often a direct result of increased inflammation and autoimmunity [21].
2) Pain and Inflammation
CRPS
Complex regional pain syndrome (CRPS) is a form of chronic pain that can be excruciating. It is worsened by SIBO, obstructive sleep apnea, and microglial activation in the brain. By keeping the microglia in a resting state and increasing endorphins, low-dose naltrexone may reduce the pain and inflammation in CRPS [23, 23].
A lot of people with CRPS experience a movement disorder called dystonia, which causes painful, uncontrollable muscle contractions. In a report, LDN lowered pain and uncontrollable muscle spasms in two people with CRPS. It worked by reducing the activation of microglia that trigger inflammation and pain [24].
LDN may also enhance the pain-relieving effects of acupuncture, which people with CRPS would benefit from. LDN alone increases the number of receptors for opioids and cannabinoids, which boosts the response to these calming, inflammation-reducing, and pain-relieving natural substances. Combined, these two modalities achieve greater synergy [25].
Pain and Seizure Relief
Low doses of naltrexone may enhance the pain-relieving and seizure-reducing effects of cannabinoids and opioids. In one study of 10 people, ultra-low-dose naltrexone enhanced the painkilling effect of an opioid drug (buprenorphine: naltrexone ratio of 166:1). Such an effect is not surprising since naltrexone increases natural opioids [26].
In mice, LDN increased the anti-seizure effects of opioids and cannabinoids. These findings suggest that it may help people with epilepsy, especially those who use medical cannabis [27].
In addition, LDN reduced the tolerance to morphine in another study in mice. Constantly having to up opioid dosage due to tolerance is a big issue, and it increases the risk of serious adverse effects. Low doses of naltrexone may help people with severe pain stay who require opioids stay at a lower dose over a longer period of time [28].
Nerve Inflammation
Transverse myelitis is an inflammation of the spinal cord that can severely damage nerve insulation (myelin). It also causes nerve pain that rarely responds to any medication [29].
In one case report, a person with such spinal cord inflammation who previously didn’t get relief from painkillers and immune therapies experienced pain relief with LDN (3 – 4.5mg/day). Low naltrexone doses probably worked by reversing microglial activation, which reduced nerve inflammation and pain. Additionally, LDN allows anti-pain pathways to re-wire by boosting endorphin production [29].
Inflammatory Gut Disorders (IBS and IBD)
Irritable Bowel Syndrome (IBS) can have many hidden causes, but stress, inflammation, and autoimmunity are often a large part of it.
In one study of 42 people with IBS, ultra-low doses of naltrexone (0.5 mg/day) increased the number of pain-free days and provided overall symptom relief in 76% of the cases. It reduced abdominal pain, stool urgency, consistency, and frequency after just 4 weeks. Importantly, LDN was safe and didn’t cause any side effects [30].
Similarly, multiple studies have shown that low-dose naltrexone can help relieve symptoms of Irritable Bowel Disease (IBD). IBD encompasses Crohn’s and ulcerative colitis [31].
According to one analysis, LDN may help people with Crohn’s disease. The data is limited and involves only 48 people, but the results are promising. In one study, LDN greatly reduced symptoms and disease activity of 8 people within 2 – 3 weeks. What’s more, it helped them remain stable for anywhere from 2 months to multiple years afterward [32].
In another study of 14 children with Crohn’s, LDN accomplished complete remission in one-fourth of the cases, while two-thirds improved. An 8-week course of treatment also improved their overall and social quality of life [33].
Low-dose naltrexone also offers hope for people with ulcerative colitis who don’t respond to conventional medications. In a study of 40 such severe cases with ulcerative colitis, 30% responded to this treatment and 20% experienced long-lasting benefits. Many of the long-term responders went into remission, while only 3 people relapsed [31].
Although LDN is still an experimental treatment for IBD and IBS, small clinical studies strongly speak to its potential benefits. Given its safety and profound immune-balancing effects, larger studies would further provide the support needed to establish its clinical use.
3) Cancer
LDN has been proposed as beneficial for various cancers. The list is almost endless, covering bladder, breast, colorectal cancer, brain (glioblastoma and neuroblastoma), liver cancer, lung (non-small cell), blood and bone marrow, skin, cancers of the reproductive organs, and many others.
But before LDN spurs too much excitement and is announced a “miracle cancer drug”, have in mind that much of the evidence is either anecdotal or stems from animal studies. No large-scale clinical studies have confirmed its cancer-fighting effects. What’s more, many animal and human studies used it only as an add-on to conventional treatments, or only once these treatments failed.
For example, in mice with ovarian cancer, LDN coupled with chemotherapy (cisplatin) worked as a unique, non-toxic, side-effect-reducing supportive therapy. Additionally, it increased the production of a so-called opioid growth factor, the only known natural opioid that blocks the growth of ovarian cancers and their blood vessels [34].
It’s important to note that low-dose naltrexone is very safe and does not appear to be toxic. Since standard therapy is very rough on healthy cells and can cause severe side effects, the beneficial profile and immune-enhancing action of LDN becomes key.
ALA/LDN Protocol
In one study of 10 advanced cancer patients who failed standard therapy, LDN (5mg/day) was given with alpha lipoic acid and hydroxycitrate. All patients had metastases and were considered to be at the end-of-life, non-curable stage. One patient had a great response, while this combo stabilized 5 patients and slowed down cancer progression. The 4 remaining patients still died within a short period of time [35].
Long-term survival of a person with advanced cancer treated with LDN and alpha lipoic acid (ALA) has been reported. The man had pancreatic cancer and metastases to the liver. He didn’t experience any side effects from the treatment and was alive and well almost 7 years later – far beyond expectations [36].
Three other similar pancreatic cancer cases were described. One was doing well 3 years later, the second had no evidence of disease after 5 months of therapy (PET scan detection). The third patient was an extremely complex cancer case whose remission was also confirmed after just 4 months of treatment [36]
According to this approach, the ALA/LDN protocol works in the following way [36, 37].:
ALA reduces oxidative stress, stabilizes inflammation (via NFkB), and restores the natural death pathways of altered cancer cells. It also seems capable of targeting only cancer cells, without harming any healthy cells
Low-dose naltrexone harmonizes the immune response and increases opioid receptors in tumors, making them more responsive to the growth-inhibiting effects of endorphins. All the while, it increases the number and activity of immune cells that can fight off cancer (cytotoxic T cells and natural killer cells)
One study on bone marrow cells highlights this immune-balancing effect. In low doses, naltrexone enhanced the maturation of bone marrow cells by increasing the activity of genes that code for cancer-fighting immune cells (MHC II, CD40, CD83, CD80, and CD86). It explains how LDN may work to enhance immunity in cancer patients. It may even be used to design immune-stimulating cancer vaccines in the future [38].
Dr. Bihari’s Experience
Dr. Bihari speaks of witnessing cancer remission in his patients prescribed LDN. He also observed that, in contrast, high doses of naltrexone may have the opposite effects and worsen cancer growth. Given that high doses reduce natural opioid activity, the immune system may be pulled further out of balance with them [39].
Other studies of LDN for cancer are currently in progress, some of which are funded by the National Cancer Institute. Dr. Bihari pointed out that clinical research studies are extremely expensive, especially large-scale ones. A trial of just 50 patients costs about $600,000, while a large enough study might cost $10 – 20 million [39].
He also considers that most investors will have no interest in putting aside such large sums of money for LDN cancer research, since it is essentially a cheap, old drug. Whether or not we’ll see large-scale cancer research with LDN somewhere in the world yet remains to be seen [39].
4) Fatigue & Brain Disorders
Anecdotally, low-dose naltrexone has been used to reduce fatigue or overall symptoms in people with Parkinson’s disease. In one small study of 8 people, LDN improved fatigue over 8 months without any side effects [40].
Other clinical anecdotes mention that LDN may help people with incurable degenerative illnesses such as ALS (Lou Gehrig’s Disease) and PLS. These diseases may have an autoimmune component, while natural endorphins may protect the brain from further damage. The reports from 15 ALS patients who used LDN are mixed [41]:
About half didn’t experience any effect or were unsure
One-third reported moderate efficacy
One-fifth reported slight efficacy
The benefits included balance and speech improvements, more energy and less phlegm, and easier breathing. However, these reports were subjective and un-blinded [41].
5) Autism
At first, naltrexone was used in regular, high doses, in an attempt to improve symptoms of autism in children. The opioid system and our endorphins have profound effects on social interactions, which are impaired in autism. For example, one such study used a dose of mg/kg/day, which would amount to about 15 mg/day for a 66 lbs child – way above the “low-dose” benchmark [42, 43].
The early studies did report increased endorphins and improved symptoms in autistic children who received naltrexone. The doses ranged from 5 to 50 mg/day, used every other day. A couple of researchers then discovered a better response with low doses.
Some doctors prescribe low-dose naltrexone to children with autism. However, 90% of the published studies were done with high doses. On the other hand, only low doses have the potential to boost stress resilience, social bonding, emotional well-being, mood, and immunity.
Dr. Jaquelyn McCandless, an LDN advocate, reported very positive effects of LDN formulated as a transdermal cream in children with autism after 8 weeks. Each patch contained 3mg of naltrexone and was given between 9 and 12 pm. She also included a couple of adults with Crohn’s Disease and one with Chronic Fatigue Syndrome to test the 4.5mg patch. According to her, everyone responded positively.
However, Dr. McCandless did not conduct a proper clinical study. Rather, this was a mere clinical observation. The concept of low-dose naltrexone skin patches is an interesting one. Patches are much easier to use, especially in children, while they can provide the same dose of the drug.
To sum it up, although it’s possible that LDN helps with autism, there is currently no hard evidence to prove it. On the bright side, LDN seems to be safe and some physicians do prescribe it for autism off-label while closely monitoring their patients’ responses.
6) Stress & PTSD
By increasing natural opioid activity, LDN may increase resilience to stress and fine-tune some emotional imbalances. Its immune-balancing effects may also have a positive impact on mood. For complex mental health issues, though, it should always be part of an integrated psychotherapeutic approach [44].
In one study, LDN (2 – 6 mg/day) was given to 15 people with severe trauma-related, dissociative disorders, and post-traumatic stress disorder (PTSD). It had multiple positive effects on 11 of them, improving their self-control and capacity to deal with reality in a healthy way. They reported a clearer perception of both their own body, their inner life, and their surroundings [45].
Although preliminary, low-dose naltrexone seems to positively impact the emotional and mental perception of reality, which is key for overcoming trauma and PTSD.
7) Addictions & Withdrawal
High-dose naltrexone (and naloxone) is still considered a conventional treatment for opioid use disorders. On the other hand, low naltrexone doses remain experimental. LDN may help people with addictions by boosting natural opioids and reducing the need for stronger external triggers in the long run – be it opioid drugs, cocaine, alcohol, or cigarettes.
Opioid Withdrawal and Detox
In a study that tracked 10k people, LDN improved pain tolerance and interpersonal interactions in post-detoxification patients [19].
In another study of 127 people undergoing a 6-day methadone taper, very-low-dose naltrexone (0.125 – 0.25 mg/day) with another drug (clonidine) reduced the intensity and stress of withdrawal, lowered craving, anxiety, restlessness, bone and muscle aches, and sweating [46].
Alcohol and Cigarette Craving
In one study with 130 heavy-drinking smokers, the combination of medium-dose naltrexone (25 mg/day) and the smoking-cessation drug varenicline was reduced cigarette and alcohol cravings, as well as the intensity of the “high” from both substances [47].
The naltrexone dose was relatively high: 5-fold the dose that Dr. Bihari and other clinical studies of LDN used. This initially higher dose may help stop smoking and drinking to start with, after which the dose can be lowered to boost natural opioid activity [47].
Cocaine Relapse
In rats, LDN with another dopamine-blocking drug (L-tetrahydropalmatine) prevented cocaine abuse relapse. It reduced drug-seeking behavior and increased endorphins without causing fatigue and sedation. of the rats in various scenarios. LDN specifically increased the activity of the gene that aids the production of endorphins in the body (POMC) [48].
8) HIV/AIDS
The whole concept of Low Dose Naltrexone started with HIV/AIDS patients, when Dr. Bihari noticed it enhances and rebalances a compromised immune system. To date, he administered this treatment to hundreds of people with HIV/AIDS and claims that some no longer have detectable levels of the virus in their systems [39].
According to Dr. Bihari, LDN restores otherwise low levels of endorphins in people suffering from HIV/AIDS. In return, their immune system, energy levels, and general well-being improve [39].
Since the initial research phases in the 80s, the HIV/AIDS epidemic has shifted from the North American continent to Africa. Naltrexone is a very affordable drug that may help millions of people suffering from HIV/AIDS in the developing world. In fact, LDN has already been approved in Nigeria as an AIDS treatment [49].
Dr. Bihari considers that Low Dose Naltrexone doses may also be helpful for people with other types of chronic infections, such as tuberculosis, Lyme, genital herpes, and potentially even Hepatitis C. The same rationale follows: LDN boosts healthy immunity and the ability to fight off infections.
These claims still rely only on clinical experience, and no large studies have confirmed them.
Synergies (Lifestyle & Supplements) of LDN
There are many other ways to increase your natural opioids that may work in synergy with Low Dose Naltrexone. The following will either increase the activation of your receptors, their sensitivity or boost your endorphin production:
Warm showers [50]
Social interaction [56]
Massages [57]
Acupuncture [60]
Butyrate [63]
Acidophilus probiotics [65]
LLLT [67]
Pregnenolone (only in specific cases) [69]
Depending on your health concerns and lifestyle, some of these may work better than others.
Dosage of LDN
Consult with your physician before taking Low Dose Naltrexone. This medication requires a prescription and should only be used under the guidance of a qualified healthcare professional.
Typical Protocol & Dosage
LDN is usually taken only once a day before bedtime [7].
The dosage typically ranges from 1.5 mg to 5 mg/day*.
Slow/timed-release naltrexone and LDN capsules that contain calcium carbonate filters should be avoided [7].
Pills are the most common form, but topical creams and patches have also been developed; they may work better for children or people who have difficulty swallowing.
Low Dose Naltrexone is commercially available only at a 50mg dose, which means that you need to get your prescribed low-dose formulation from a compounding pharmacy [1].
*Dr. Bihari considers that the dose should be no less than 1.75 – 2 mg/day and no higher than 4.5 – 5 mg/day. He found that 3 mg/day is a good dose that works for most people [6].
Ultra-low Dosage
This is where the confusion kicks in, as some studies used so-called “ultra Low Dose Naltrexone”, ones that range from 0.125 – 0.5 mg/day. On the other hand, borderline doses of 0.5 – 1 mg/day are simply considered “very low-dose” [3].
There is no clear benefit to very or ultra-low doses, based on the published studies. However, each person is different and your doctor may consider that doses in this range will work better for you.
Dosage Window
Despite this variance, the dosage window is small. In general, higher doses run a greater risk of stronger blockage and reduced LDN effectiveness. The ideal dose for each person is individual: it’s the dose that maximally increases the endorphins and minimally blocks them. Some people are more sensitive to the effects of LDN. In the future, it may be possible to check a person’s endorphin levels to truly personalize the treatment [1].
Drug Interactions
The only drugs LDN should not be used with are opioid painkillers (codeine, morphine, fentanyl, hydrocodone, methadone); their interaction is still not well-understood. Low doses of naltrexone may still block opioid receptors and temporarily reduce their effectiveness [7].
People who used (or abused) opioids long-term may require 10 days to 2 weeks before LDN can be started. Your doctor will be able to assess this based on your individual case.
People who have had organ transplants and are taking immunosuppressive drugs permanently are cautioned against the use of LDN.
There are no other reports of LDN interactions with other drugs.
Synergistic effects with anti-inflammatories and drugs used for treating rheumatoid arthritis are possible [7].
Side Effects of LDN
Most people didn’t experience any side effects in the published clinical trials to-date.
The side effects that have been reported are mild.
Sleep Issues
Some people experience vivid dreams (or rarely nightmares), which goes away with time. Insomnia is another possible side effect. In such cases, the dosing can be moved to the morning [7].
Dr. Bihari added that poor sleep is the only side effect he noticed in a very small percentage of people on 3 mg/day. He considers that lowering the dose is a better solution than moving it to the morning and that poor sleep just indicates an increased sensitivity to the drug. In his experience, lowering the dose from 3mg/day to 1.5 – 2 mg/day will resolve the sleep disturbance in most people [6].
Alternatively, you can discuss natural calming supplements or lifestyle adjustments to help you overcome sleep issues while on low-dose naltrexone. Some good supplements include magnesium, melatonin, and hops. Make sure to get enough sunlight during the day and block out blue light at night.
All in all, insomnia is quite rare with LDN. Most people say their sleep quality improves [7].
Other
According to the published studies, mild headaches are also possible. Increased anxiety has been reported by some physicians, but this was mostly in people undergoing opioid withdrawal and probably not related to naltrexone [7].
There are anecdotes of people with CFS and mold illness not reacting well to LDN. This could also possibly be due to increased sensitivity. If you fall under this category, speak to your healthcare practitioner.


© 2004 - 2026. All rights reserved. Benjamin McAvoy Integrative Naturopath
Visit
Settlers Blvd
Chisholm NSW 2322
Australia
Hours
Mon – Fri
9.30am – 4.30pm
Alt. Sat 9am – 12pm
Integrative Naturopath, Iridologist and Medical Herbalist Chisholm, NSW. Serving clients in-clinic and via tele-health worldwide.